

Background: Contemporary trials in adult Ph+ ALL patients with TKIs continue to show improved outcomes with allogeneic blood or marrow transplantation (alloBMT) in first remission (CR1) (Chalandon. Blood. 2015 AND Ravandi. Blood Adv. 2016). These studies have relied on myeloablative conditioning (MAC) and largely required an HLA-matched donor. Post-transplant survival in Ph+ ALL has been shown to be similar between patients transplanted with reduced-intensity conditioning (RIC) and MAC, but the incidence of relapse after RIC is higher (Bachanova. Leukemia. 2014). Post-transplant TKI maintenance reduces the incidence of relapse (Brissot. Haematologica. 2015), but this strategy has not specifically been investigated after RIC. Additionally, HLA-haploidentical donor transplants using post-transplant cyclophosphamide (PTCy) as a component of graft-versus-host disease (GVHD) prophylaxis have comparable outcomes to HLA-matched transplants (McCurdy. Haematologica. 2017). We analyzed outcomes among patients who universally received PTCy and attempted post-transplant TKI prophylaxis to determine the importance of remission status (CR1 vs. later), conditioning regimen, donor type, and TKI choice.
Methods: The bone marrow transplant database at Johns Hopkins was queried for adult patients with de novo Ph+ ALL who received alloBMT using PTCy between January 2008 and August 2018. Characteristics of patients were summarized and compared using the student's T test for continuous variables and Fisher's exact test for categorical variables. Estimators of OS and RFS were reported using the Kaplan-Meier method. Differences in time-to-event outcomes were estimated using Cox proportional hazards model.
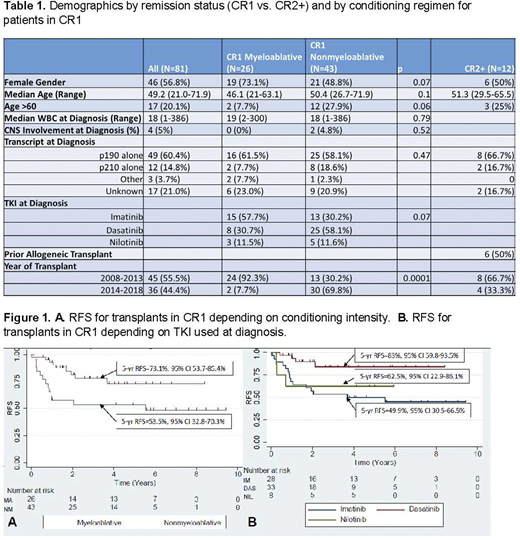
Results: A total of 81 transplants for Ph+ ALL were performed: 69 (85%) in CR1 and 12 (15%) in second or greater remission (CR2+). The demographics are presented in Table 1 and separated by conditioning regimen [MAC vs. nonmyeloablative (NMAC)] for transplants in CR1. The cumulative incidences of grade 2-4 and grade 3-4 aGVHD at 1 year were 33% (95% CI, 23% to 44%) and 9% (95% CI, 3% to 15%), respectively. The incidence of moderate or severe cGVHD at 2 years was 8% (95% CI, 2% to 13%). Nearly all patients (91.4%) initiated a post-transplant TKI at a median of 56 days. Overall, 44.4% of patients were able to take a TKI on ≥85% of nonrelapse days from day 31-395 post-transplant.
AlloBMT in CR1 (compared to CR2+) improved RFS (HR=0.25, p=0.0002) and pre-transplant minimal residual disease (MRD) by flow cytometry (MFC) was associated with decreased RFS (HR=2.57, p=0.039). The presence of pre-transplant MRD by PCR did not confer an increased risk of relapse (HR 1.12, p=0.84). Among the 69 patients transplanted in CR1, the 5-year OS was 77.6% (95% CI, 64.8% to 86.2%) and RFS was 67% (95% CI, 52.4-76.5%). As shown in Figure 1, the use of NMAC versus MAC (HR 0.37, p=0.02) and dasatinib versus imatinib at diagnosis (HR 0.21, p=0.007) led to improved relapse-free survival (RFS) in univariate analyses. Neither donor type (with the majority being haploidentical) nor recipient age ≥60 affected RFS. Post-transplant TKI prophylaxis was discontinued prior to relapse in 20 patients among whom 12 remain in an MRD-negative remission, 4 died of non-relapse causes, 3 relapsed, and 1 developed recurrent MRD controlled by a TKI. The median duration of post-transplant TKI prophylaxis prior to discontinuation was 46.5 months in those who remain in treatment-free remission versus 15.6 months in those who relapsed (p=0.01). Eighteen relapses occurred on maintenance therapy, and 90% of tested cases were positive for a kinase domain mutation conferring resistance to the TKI in use at relapse. No significant difference in the median time to TKI initiation post-transplant was noted between those who relapsed on maintenance and those who did not (70 days vs. 55 days, p=0.6). All patients in ongoing remission were MRD-negative by PCR at their most recent evaluation.
Conclusions: AlloBMT with PTCy in Ph+ ALL was most effective when performed in CR1 with negative MFC for MRD. The initiation of post-transplant TKI prophylaxis was nearly universal. Among patients transplanted in CR1, the best results were achieved in patients treated with dasatinib at diagnosis (5-year RFS 83%) and NMAC (5-year RFS 73.1%). Thus post-transplant TKI prophylaxis appeared to overcome any relapse control advantage for MAC, yielding better outcomes with NMAC.
Webster:Amgen: Consultancy; Pfizer: Consultancy. Luznik:WindMil Therapeutics: Patents & Royalties: Patent holder; Genentech: Research Funding; Merck: Research Funding, Speakers Bureau; AbbVie: Consultancy. DeZern:Abbvie: Consultancy; Astex: Research Funding; MEI: Consultancy; Celgene: Consultancy, Honoraria. Pratz:Jazz Pharmaceutical: Consultancy; Millennium: Research Funding; Daiichi Sankyo: Research Funding; Agios: Other: Scientific Advisory Board, Research Funding; Celgene: Other: Scientific Advisory Board; Boston BioMedical: Consultancy; Astellas: Other: Scientific Advisory Board, Research Funding; AbbVie: Other: Scientific Advisory Board, Research Funding. Levis:Astellas: Honoraria, Research Funding; Menarini: Honoraria; Amgen: Honoraria; FujiFilm: Honoraria, Research Funding; Daiichi-Sankyo: Honoraria. Gojo:Amgen: Research Funding; Merck: Research Funding; Genentech: Research Funding; BMS: Membership on an entity's Board of Directors or advisory committees; Amphivena: Research Funding. Bolanos-Meade:Incyte: Other: DSMB Fees. Dalton:Eli Lilly: Research Funding; AbbVie: Research Funding. Jain:Takeda: Consultancy, Honoraria; Bristol Myer Squibb: Other: for advisory board participation; CareDx: Other: Advisory Board. Ali:Celgene: Membership on an entity's Board of Directors or advisory committees. Borrello:Celgene: Research Funding; Aduro: Patents & Royalties; WindMIL Therapeutics: Other: Founder , Research Funding. Wagner-Johnston:ADC Therapeutics, Regeneron, CALIB-R, Verastem: Membership on an entity's Board of Directors or advisory committees. Smith:Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Agios: Consultancy, Membership on an entity's Board of Directors or advisory committees; Jazz: Consultancy, Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal